标题:Supplementation with Riboflavin (Vitamin B₂) for Migraine Prophylaxis in Adults and Children: A Review
**Abstract**:
**Key words**: riboflavin; migraine; adult; child
The exact mechanism of migraine is unknown, but it seems that an interaction between genetic and environmental factors leads to migraine attacks [10]. Neuronal factors, blood vessels, and high levels of serotonin are involved in this type of headache [11]. Concern about the potentially adverse effects of medications results [12] in a high tendency to treat migraine attacks with alternative medicines such as vitamin and mineral supplements [13]. Some dietary supplements that can alleviate migraine symptoms include magnesium [14 – 15], carnitine [15], niacin, tryptophan, and riboflavin [13]. Riboflavin (vitamin B₂) is a precursor of flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD), both of which play key roles in the electron transport chain and energy production in the mitochondria [13]. When there is a decrease in the reserved energy in mitochondria of the brain, biochemical shifts involved in activation of the trigeminovascular system lead to a migraine attack. There is a theory that associates low riboflavin levels with the occurrence of migraine attacks [16]. Low vitamin B₂ leads to mitochondrial dysfunction and oxygen metabolism disorders. This dysfunction may have an effect on migraine pathogenesis [16 – 17]. The aim of the present study was therefore to carry out a literature review to summarize the effects of vitamin B₂ supplementation on migraine prophylaxis in adults and children.
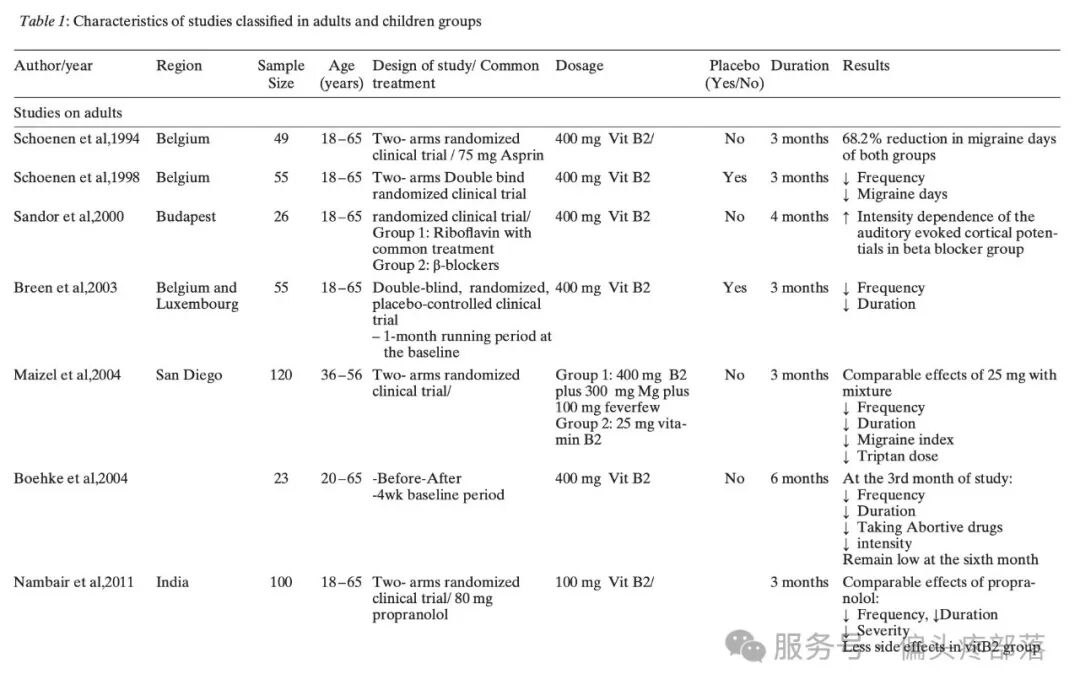
Maizels et al. compared a combination of riboflavin 400 mg, magnesium 300 mg, and feverfew 100 mg (Intervention 1) with 25 mg riboflavin (Intervention 2) in patients with migraine of both sexes and with a mean age of 46.8 years old in San Diego. They indicated that intervention 1 was no more effective than riboflavin at 25 mg/day in the reduction of migraines (42 % vs. 44 %), migraine days (33 % vs. 40 %), frequency (7.8 % vs. 7.7 %), and migraine index (13.3 % vs.14.1 %) after a three-month intervention [19]. A migraine index is calculated by multiplying the intensity and frequency of attacks and the duration of a migraine headache. It seems that there is an unidentified interaction between the three ingredients in the intervention group which could prevent the effects of riboflavin at doses of 400 mg, which was reported as a limitation of the study. The compliance of patients was also not recorded.
Breen et al.’s study was a double-blind, placebo-controlled clinical trial which was conducted on 55 Belgian patients with migraines, of both sexes and an average age of 36 years. They indicated that a high dose of vitamin B₂ (400 mg/day) resulted in three fewer migraine days, a reduction in severity on the 4-point scale, migraine index, duration, and nausea or vomiting compared to the placebo group after three months (p < 0.05 in all variables). The number needed to treat (NNT) was 2.8 in order to decrease the frequency of migraine attacks by 50 % [20]. This means that according to the Breen et al. study three patients need to be treated with 400 mg/day of vitamin B₂ in order to decrease the frequency of migraine attack by 50 % in one patient. Baseline characteristics and quantitative data were not reported in this study.
Schoenen et al. compared the effects of 400 mg/day riboflavin with the same dose combined with 75 mg/day aspirin in Belgian subjects with migraine. Migraine severity decreased in both groups. No significant differences were observed between the rating of subjective improvement and the recorded number of migraine days (8.7 ± 1.5 days vs. 8.9 ± 2.2 days). The clinical response did not differ significantly between the two groups. According to Schoenen et al., supplementation with 400 mg/day of riboflavin was comparable to aspirin combined with riboflavin in the reduction of migraine duration. Comparison within groups indicated a significant reduction in migraine days in the riboflavin group (baseline: 8.7 ± 1.5; end: 2.9 ± 1.2 days) after three months in Belgian patients [21]. In this study, participants and researcher were not blinded to the intervention and the general characteristics of the study subjects were not presented.
Although propranolol is a common medication in migraine prophylaxis, it has side effects and is not well-tolerated by a large number of patients. In a six-month study, Nambiar et al. compared a lower dose (100 mg) of vitamin B₂ with 80 mg/day of propranolol in Indian patients with a mean age of 31 years. The study groups were matched based on sex and age. At baseline, no significant differences were observed in the frequency, duration of attack, or other general characteristics. At the end of the first month, there were significant differences between the two groups in the frequency of headaches (3.3 ± 0.6 in the propranolol group vs. 3.9 ± 1.0 in the riboflavin group), but at the end of the sixth month, no differences in the frequency of migraines (2.8 ± 0.7 vs. 2.9 ± 0.7) or duration of headaches over an hour (2.9 ± 1.0 vs. 2.6 ± 0.8) were observed. The authors concluded that the positive effects of vitamin B₂ were comparable to those of propranolol in the frequency, severity, duration of attacks, and disability at the third and sixth month of the intervention. They also suggested that 100 mg/day of riboflavin is a well-tolerated and safe supplement in migraine prevention [22].
In a trial by Boehnke et al., 23 German patients with migraine were recruited after a four-week run-in period. They received 400 mg of vitamin B₂ per day for five months. After three months of treatment, the frequency of migraines in the participants was reduced significantly from four days to two days/month and remained low at 2 attacks/month after six months. Abortive medications were decreased from 7 to 4.5 units/month without any side effects. The duration of migraine attacks was 50 hours at the baseline and was reduced significantly to 22 – 28 hours at the end of the study. Migraine intensity was not affected, however [23]; this was 3.3 at the baseline and no significant changes were observed after three and six months of the intervention (3.0 at the end of the study). Participants reported no serious side effects throughout the study. This was a before-after study with no control group.
Schoenen et al. performed a pilot study on 25 Belgian patients with migraines. A 68 % reduction in migraine intensity was observed in participants. As a result of this pilot study, they designed a randomized clinical trial for 55 subjects. A comparison of 400 mg/day of riboflavin with a placebo indicated a reduction in frequency and days of migraine attacks with no serious side effects. The proportion of participants who improved by at least 50 %, was 15 % for the placebo group and 59 % for the riboflavin group (p < 0.01). NNT was 2.3 for 50 % improvement [24]. As with the other studies, participants did not report any serious side effects.
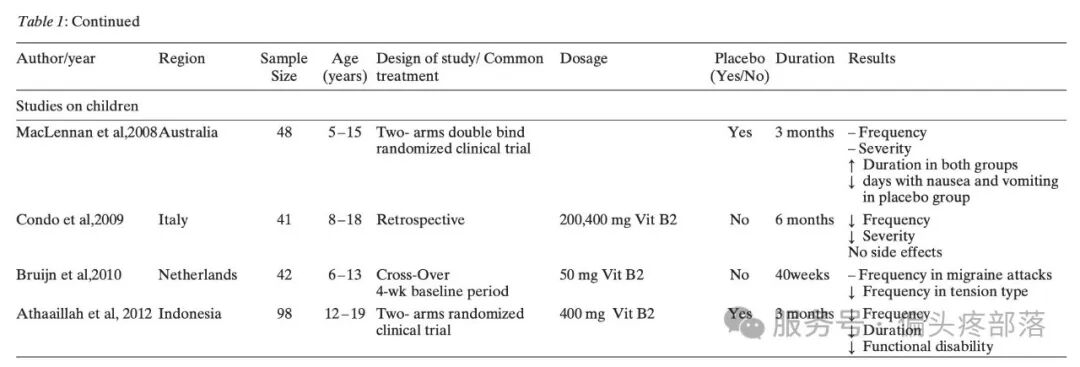
In Athaaillah et al.’s double-blind randomized controlled clinical trial, adolescents with a mean age of 14.5 years received 400 mg/day of vitamin B₂ for three months. In the second and third months, the duration and frequency of migraines were reduced. The frequency days mean in the riboflavin group was 6.4 ± 2.0 day which reduced to 3.7 ± 1.28 days at the end of the trial. A migraine attack duration of more than two hours was observed in 38 % of participants in the riboflavin group, but after the intervention, no one reported attacks lasting more than 2 hours. A PedMIDAS questionnaire indicated a significant reduction in functional disability in the intervention group compared to the placebo group [27].
In a retrospective study on 41 Italian adolescent and pediatric patients with a mean age of 13 years, Condo et al. compared taking 200 or 400 mg/day of vitamin B₂ for six months. They divided their study into the following three-month periods: a baseline period without prophylactic medications (Phase 1), riboflavin treatment (Phase 2), and follow-up after the suspension of vitamin B₂ (Phase 3). For patients who consumed riboflavin for four or six months, and evaluated the last three months of therapy, Phase 2a (2nd, 3rd, and 4th month) and Phase 2b (4th, 5th, and 6th month) were considered. Fifty percent or more improvement was observed in the frequency and intensity of migraines in 68.4 and 21 % of participants (p < 0.05 in both variables) who took 200 mg/day riboflavin. The mean attack frequency in Phase 2 decreased significantly compared to the baseline (21.7 ± 13.7 vs.13.1 ± 11.8). Headache intensity also decreased from 2 ± 0.5 in Phase 1 to 1.6 ± 0.8 in Phase 2, and its reduction continued to Phase 3. No differences were found in migraine intensity in Phases 2a and 2b. Mild side effects (vomiting and an increase in appetite) were reported in two subjects [28].
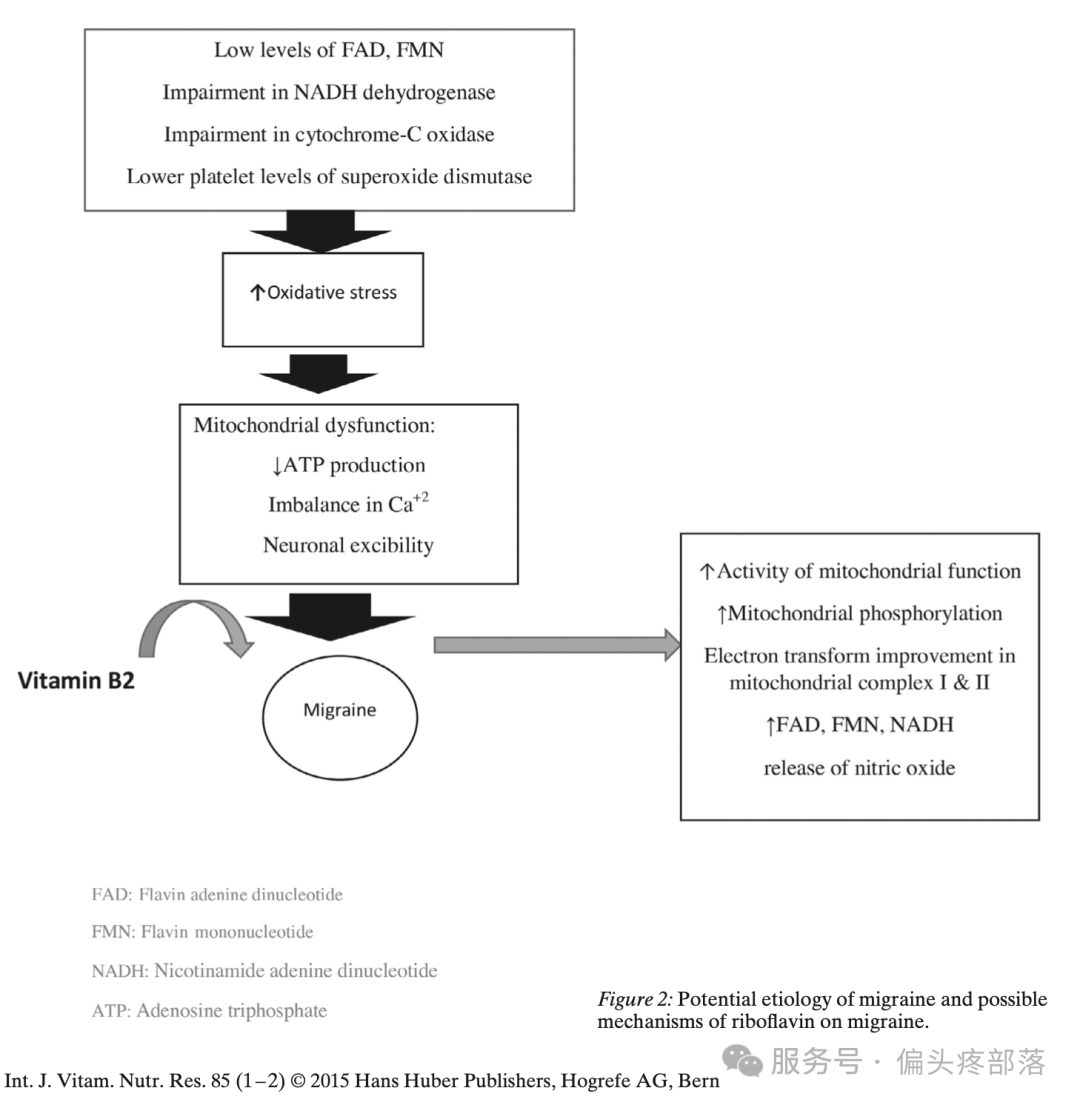
Riboflavin is a water-soluble vitamin that participates in transferring electrons in mitochondrial oxidation-reduction reactions [19]. In some diseases such as lactic acidosis, stroke-like episodes (MELAS), mitochondrial encephalomyopathy, and migraine, the metabolism of energy decreases in mitochondria. It has been hypothesized that riboflavin increases complex I and II activity and energy metabolism [16]. The potential mechanisms of vitamin B₂ on migraine are shown in Figure 2. As presented in the figure, several factors including low levels of FAD, FMN, impairment in NADH dehydrogenase or cytochrome-C oxidase, and lower platelet levels of superoxide dismutase trigger oxidative stress. Increased oxidative stress disturbs mitochondrial functions and migraines can occur. Some potential mechanisms for the effects of vitamin B₂ on migraine are as follows: 1) increasing mitochondrial function activity and phosphorylation, improvement in electron transform in mitochondrial complex I & II, enhancement of FAD, FMN, NADH, and nitric oxide release [29 – 31].
The effects of various doses of riboflavin (400, 100, 50, and 25 mg) were studied in adults and children. According to the previous studies, an approximately 100-fold higher dose than the average dietary intake of riboflavin was tolerated well with no serious adverse effects. Previous studies compared the effects of vitamin B₂ with a placebo or low dose of riboflavin. Response to a placebo was observed in numerous studies. Schoenen et al. reported that 2.3 patients need to be treated with riboflavin in order to prevent a migraine attack in one subject [21]. Although the NNT of valproate was 1.6, it has shown serious side effects in patients with migraine [10]. In Nambiar et al.’s study, propranolol showed a faster and greater reduction in the frequency of migraine attacks, compared to vitamin B₂. This may be due to the fact that propranolol has different effect sites than vitamin B₂. The effect site of vitamin B₂ is the mitochondria and the effects on mitochondrial energy metabolism are slower than the receptor blockade. Some possible mechanisms of vitamin B₂ on migraine severity are its antinociception and anti - inflammatory characteristics, it also causes the release of nitric oxide [22].
Differences in baseline characteristics, dose, common medications, duration of intervention, methodology, and ethnicity may lead to the different efficacy of riboflavin in migraine symptoms. Only two of seven clinical trials in adults were double - blind randomized placebo - controlled clinical trials. Due to limited high - quality studies on the effects of vitamin B₂ on migraine in adults, drawing a definite conclusion is not possible.
There are limited studies about the effects of vitamin B₂ on migraine in children. The beneficial effects of riboflavin were only observed in two out of three randomized clinical trials and one observational study. Several limitations are observed in these studies. All studies except Athaaillah et al. [27] had a small sample size; therefore, they cannot be representative of migraineurs. In the Condo et al. study, due to the absence of a placebo group, the placebo response rate which was reported in many migraine studies was not clear [28]. A high placebo response rate was observed in two studies.
Differences in dosage and age ranges make it difficult to determine the prophylactic effects of vitamin B₂ among children. Additional studies with the same dosage and age range are suggested in order to clarify the efficacy of riboflavin on migraine episodes. The dose of riboflavin used in children was relatively low compared to the dosage used in adults. Considering the higher metabolic rate of children compared to adults, the prescribed dosage of vitamin B₂ should be higher than for adults in order to produce similar effects [26].
Limitations of the present study are the lack of quantitative data synthesis and limited number of inclusion studies for both adults and children which may not provide a comprehensive review of the situation.
In conclusion, all studies in adults demonstrated the safe and well - tolerated effects of vitamin B₂ supplementation on migraines, but due to limited high - quality studies of the effects of vitamin B₂ on migraine in adults, more double - blind randomized placebo - controlled clinical trials are needed to confirm the positive prophylactic effects of vitamin B₂. Most studies examined a high dose of vitamin B₂ (400 mg) and there is not enough evidence of the effects of low and moderate doses of riboflavin in migraine headaches. Limited and non - homogeneous studies on children could not answer the question of vitamin B₂ efficacy in migraine attacks among children and adolescents. Overall, although the findings of this review suggest that a high dose of vitamin B₂ is safe in adult patients with migraine, to date there is insufficient evidence to make recommendations for its use as an adjunct therapy for adults and children.
## Conflicts of Interest
The authors declare no conflict of interest.